
A Wider Lens for Anxiety: Integrative Psychiatry After Panic Escalation
When Anxiety Starts Feeling Bigger Than the Panic Attack Itself
📌 Key Takeaways
Panic is only one signal; lasting anxiety needs a wider look at body, sleep, stress, history, and support.
Look Beyond Panic: A whole-person review can show what is driving anxiety after the episode ends.
Track Daily Changes: Avoidance, poor sleep, and fear of another attack can shape life more than panic intensity.
Respect Body Signals: New or worrying physical symptoms may need medical review before assuming anxiety is the cause.
Protect Patient Choice: Collaborative care keeps treatment tied to personal goals, comfort, and real-life capacity.
Match Care To Fit: Therapy, medication review, wellness support, or ketamine evaluation may fit different needs.
Wider care starts by seeing the full person, not just the panic.
People recovering from panic escalation will gain clearer next-step language here, preparing them for the detailed overview that follows.
The panic passed.
Now the phone feels cold in your hand. A half-finished glass of water sits on the nightstand. The room is quiet, but your body still feels on alert.
Maybe the panic attack itself lasted a few minutes. The questions afterward can last much longer. Why did that happen? Is something medically wrong? Why does sleep feel different now? Why does commuting, work, or being alone suddenly feel harder?
If that describes where you are right now, this article is written for exactly that moment. Not the moment during the attack, but the confusing stretch afterward, when symptoms have quieted but anxiety hasn't, and when the pieces don't quite add up into a clear picture.
This is an educational resource, not emergency guidance. If you are currently in crisis or believe you may be in immediate danger, call 911 or go to the nearest emergency room. If you are in emotional distress, call or text 988 for the Suicide & Crisis Lifeline, or contact NYC 988 for free, confidential mental health support available 24/7 in more than 200 languages. New York Integrative Psychiatry is not an emergency resource and does not offer after-hours or emergency assessments.
For those who are past the acute moment and trying to understand what comes next, there is a frame worth introducing early: the idea of a wider clinical lens. A panic episode is real and significant, but it is rarely the whole story. Symptoms, sleep, stress, body signals, life history, and care preferences can all shape what a person actually needs; a narrow focus on the episode alone may leave many of those pieces unexamined.
Integrative psychiatry after panic escalation means looking beyond the panic episode alone. A whole-person evaluation may consider symptoms, body signals, sleep, stress, life history, functioning, medication questions, therapy needs, and personal goals so the care pathway fits the person rather than forcing every anxiety experience into one treatment lane.
What Integrative Psychiatry Means in Anxiety Care
Integrative Psychiatry is a whole-person psychiatric approach that considers symptoms, biology, medication options, lifestyle, therapeutic context, and personal goals together — rather than isolating one variable as the primary target. Think of it as widening the lens from a single symptom to the full picture of a person's health and life.
The phrase "a collaborative path toward wholeness" captures the orientation well. This approach honors the full complexity of who a person is. It bridges evidence-based psychiatric care — including psychopharmacology and psychotherapy — with careful attention to mind, body, and broader life context. Depending on what a thorough evaluation reveals, a whole-person care pathway may include precision medication management, psychotherapy, nutritional psychiatry, somatic and mindfulness-based practices, lifestyle interventions, trauma-informed care, or, where clinically relevant, in-person ketamine evaluation.
That list is not a treatment protocol for every person who walks through the door. It describes what the lens can see. The aim of an integrative psychiatric evaluation is to understand which of those dimensions actually apply to your situation — and to build a plan that fits your goals, preferences, history, and capacity to begin.
What integrative psychiatry is not: a rejection of conventional medicine, a promise of any particular outcome, or an automatically medication-light approach. It is a more complete form of evaluation that starts with curiosity rather than assumptions. The care is collaborative and personalized, aligned with the patient's goals rather than with a predetermined script.
Why Panic Intensity Alone Does Not Explain the Whole Picture
The severity of a panic attack matters, but it does not determine what kind of care fits next.
A single intense episode may feel less disruptive if you recover quickly and return to normal routines. A less dramatic episode may still become life-shaping if you start avoiding the subway, canceling plans, checking your pulse repeatedly, or sleeping poorly because you are afraid it will happen again. The question that matters is not only "how intense was the panic?" but "what else is shaping this pattern?"
The National Institute of Mental Health describes panic disorder as involving repeated unexpected panic attacks along with physical symptoms such as chest pain, heart palpitations, shortness of breath, dizziness, or abdominal distress. A single severe episode can feel like a medical emergency, which is why medical evaluation is often a sensible first step when physical symptoms are new or concerning. But the intensity of the episode alone doesn't tell you everything you need to know about what kind of care fits next.
Consider what the weeks around a panic escalation often involve: sleep disruption that started before or deepened after the episode; a stress load that had been accumulating quietly for longer than it felt; physical sensations that linger in ways that are hard to name; work strain or relationship tension that predated the attack; a growing instinct to avoid certain places — crowded trains, unfamiliar environments, situations that now feel unpredictable rather than manageable.
Anxiety disorders can involve biological, psychological, lifestyle, relational, and contextual factors operating simultaneously. Current coping tools may feel insufficient without being obviously broken. Medication questions may have surfaced for the first time. Trauma or chronic stress that lived in the background may now feel more present and harder to ignore.
A broader clinical lens can help organize those signals into a clearer picture of what you are actually dealing with, and what level of support makes sense. Physical symptoms always deserve appropriate medical evaluation. This article cannot assess what is medically urgent for any individual, and if you have new, severe, or concerning physical symptoms, please seek evaluation from a healthcare provider before drawing conclusions about their cause.
The Whole-Person Evaluation Map
The table below is a conversation-preparation tool, not a diagnostic checklist. Its purpose is to help you organize what you are noticing — before or during a clinical conversation. A clinician is the appropriate person to interpret this information. The map's job is to help you arrive at that conversation with more clarity, better questions, and a fuller picture of what you want to understand.
| Area to Explore | Why It Can Matter | Questions to Bring Into Care |
|---|---|---|
| Panic and anxiety pattern | Helps clarify timing, recurrence, triggers, and fear of recurrence. Understanding when symptoms began, whether episodes have repeated, and what tends to precede or follow them shapes a meaningful evaluation. | When did this start? Has it happened before? What does the pattern look and feel like before, during, and after? |
| Body signals and medical-safety questions | Physical symptoms can overlap with anxiety and medical concerns. Integrative psychiatry does not treat the body as separate from the mental health picture. Body signals deserve organization, not minimization. | Are there physical symptoms that feel concerning or new? Has a medical evaluation been completed? |
| Sleep and nervous-system load | Sleep disruption is among the most common contributors to anxiety intensity. Caffeine, substances, and cumulative stress load also shape how the nervous system responds to uncertainty. | How has sleep changed? What has the stress level been for the past several weeks or months? |
| Stress, work, and environment | Living in a dense, high-demand environment can create a sustained baseline of nervous-system activation. New York's pace, commuting demands, and work culture can compound anxiety in ways that don't always get acknowledged in a clinical conversation. | What changed in your environment around the time the anxiety escalated? |
| Life history, trauma, and relational context | Anxiety can be shaped by lived experience, stress patterns, and relationships. Sometimes a panic episode is the moment someone realizes they have been carrying more stress than they thought. | Are there past experiences, losses, or relational stressors that feel connected to what is happening now? |
| Functioning and avoidance | Changes in daily functioning — avoiding the subway, canceling plans, struggling through the workday, losing sleep, needing reassurance before leaving home, or feeling afraid to be alone — can signal that anxiety is reshaping behavior in ways worth addressing. | What have you stopped doing or started avoiding since the panic escalation? |
| Medication history or concerns | Medication questions are among the most common reasons people feel uncertain about reaching out. Whether the concern is about starting medication, stopping it, or reviewing what is currently prescribed, this is a legitimate part of the clinical conversation. | What questions do you have about medication? What would you want a clinician to understand about your history with it? |
| Therapy needs and goals | Psychotherapy can support self-awareness, emotional resilience, and pattern recognition in ways that medication alone does not address. Clarity about what you want from therapy helps narrow the fit. | Have you tried therapy before? What worked or didn't? What do you want to understand, not just reduce? |
| Wellness supports | Sleep, nutrition, movement, and stress regulation can all influence how anxiety presents and recovers. Identifying what is and isn't working in your current routine is useful clinical information. | Which wellness practices feel supportive right now? Which feel depleted or unavailable? |
| Care preferences and capacity | Your goals, fears, readiness, and logistical constraints all shape what a care pathway can realistically look like. A plan that doesn't fit your life is unlikely to hold. | What would make care feel safe enough to begin? What are you most worried about? |
Symptoms and Panic Patterns
Start with the pattern, not the conclusion.
Understanding the timeline and pattern of your symptoms is one of the first things a clinical evaluation may explore. When did the anxiety escalation begin? Has something similar happened before, or does this feel like a new experience? What tends to happen before, during, and after an episode; has the fear of another episode already begun to change your behavior?
The National Institute of Mental Health notes that panic disorder not only involves repeated panic attacks, but is often accompanied by persistent worry about future episodes or significant behavioral changes related to the attacks. Whether or not that description fits your experience precisely, the pattern of your symptoms is meaningful clinical information. It is not a verdict about what is wrong — it is a starting point for understanding what might need attention.
The "after" matters as much as the episode itself. Some people feel physically drained. Some feel embarrassed. Some become afraid of the next episode and begin scanning for physical sensations every few minutes. That monitoring can make daily life feel narrow, and it can take hold long before a second episode occurs.
Body Signals and Medical-Safety Questions
Integrative psychiatry does not separate the body from the mental health evaluation.
After panic escalation, body sensations can become hard to interpret. A racing heart, tight chest, dizziness, nausea, tingling, shaking, or shortness of breath may occur during panic, but similar sensations can also raise legitimate medical questions, and an article cannot tell the difference for your situation.
Anxiety, stress physiology, medication effects, sleep disruption, and physical health questions can all overlap in ways that matter for care. The language that applies here is deliberate: physical symptoms "can overlap" with anxiety, they "may be connected," and they "should be evaluated when concerning" — not assumed away.
Avoid the instinct to attribute all physical sensations to anxiety without appropriate medical evaluation. New or severe physical symptoms warrant professional assessment before conclusions are drawn about their cause. Mental health care should not ask you to dismiss the body.
Sleep, Stress, Nutrition, Substances, and Nervous-System Load
The nervous system does not operate in a vacuum.
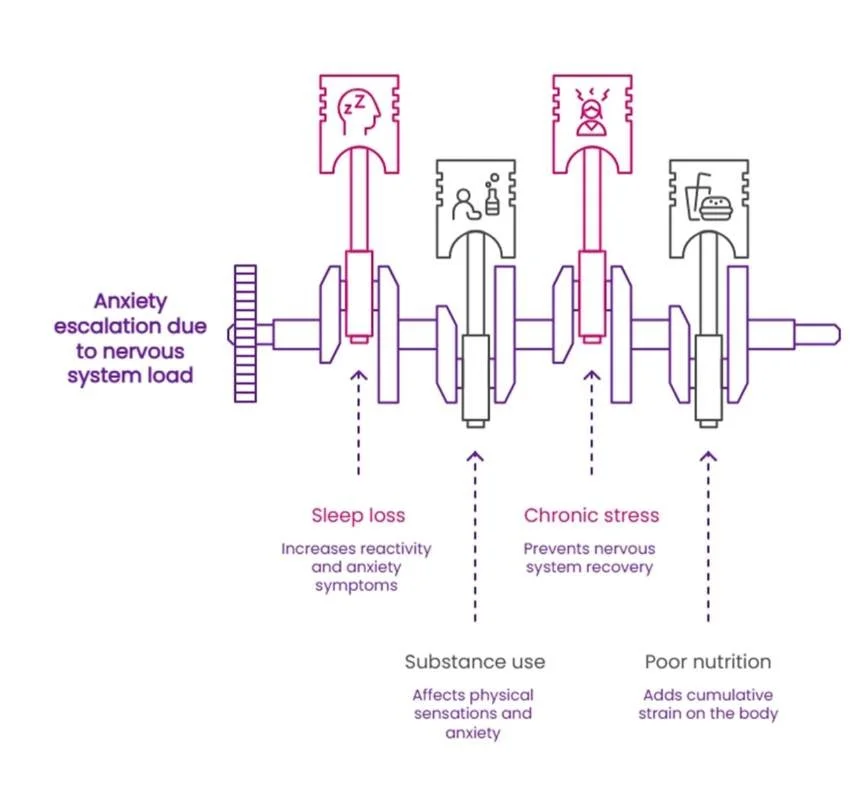
Sleep quality, caffeine and alcohol intake, substance use patterns, chronic stress, and nutritional factors can all influence how anxiety presents and how the body recovers after a panic episode. These are not lifestyle details separate from the "real" psychiatric question; they are part of it. A whole-person evaluation considers what the nervous system load is before interpreting the symptoms resting on top of it.
Sleep loss can make the next day feel more reactive. Caffeine or substances may affect some people's physical sensations. A difficult work week can make the body feel as if it never fully powers down. Eating irregularly, skipping meals, or running on adrenaline through a packed New York day can add cumulative strain.
A clinician may ask about sleep, caffeine, alcohol, cannabis, stimulants, nutrition patterns, movement, screen use, and stress load because those details can influence anxiety care planning. The goal is not to blame you for symptoms. The goal is to understand the conditions your nervous system has been living under.
Sometimes a panic episode is the moment someone realizes they have been carrying more stress than they thought. That does not mean stress caused everything. It means stress belongs in the conversation.
No specific supplement or intervention recommendations are appropriate to include here. A clinician can help identify which wellness dimensions are most relevant to your particular situation and how they fit into a broader care plan.
Life History, Trauma Context, and Relational Stress
Anxiety is inextricably tied to your lived experience.
A whole-person evaluation may explore recent losses, relationship strain, caregiving pressure, work stress, identity changes, trauma history, family patterns, and major transitions. These factors may not explain every element of a panic episode. They can still shape how safe or unsafe the world feels afterward.
Anxiety does not always announce its origins clearly. Sometimes a panic episode surfaces in someone whose external life looks stable, but whose internal stress load — shaped by past experiences, relational patterns, or accumulated losses — has been building quietly for a long time. Trauma history, attachment patterns, and ongoing relational stress can all shape anxiety in ways that a purely symptom-focused approach may miss.
The point is not that every panic attack is rooted in trauma. It is that life context deserves a place in the clinical picture — and that a whole-person evaluation creates room for that conversation.
Functioning, Avoidance, and Self-Trust
Functioning matters — not as a measure of whether someone is handling things well enough, but as a window into how anxiety is currently organizing daily life.
If you have started canceling plans, avoiding crowded places, struggling through work, losing sleep to reassurance-seeking, or feeling afraid to be away from home, those changes are worth naming. They do not mean you are failing. They mean the anxiety pattern is affecting your life.
Consider what that reorganization can look like in New York. After a single panic episode on a crowded platform, the platform itself can become a problem. Someone may start leaving twenty-three minutes early for the train, switch routes, grip the railing, and check the exits before the train arrives. The episode may be over, but life has begun organizing around the fear of another one. That is clinically relevant information — not because it reveals how intense the panic was, but because it shows what anxiety is costing in daily functioning.
A crowded subway car, a packed elevator, a loud restaurant, or a demanding workday can each become a test you never agreed to take. The city does not always leave much room to recover quietly, and those costs add up. Care may help restore the orientation, capacity, and self-trust that panic escalation can quietly disrupt.
How Collaborative Treatment Planning Protects Agency
Collaborative treatment planning protects the patient's agency — and it is the direct answer to one of the most common fears about reaching out for psychiatric care.
Many people hesitate because they worry about losing control: being reduced to a diagnosis, being pushed toward medication before the full picture is understood, or receiving a predetermined solution that doesn't fit. In a collaborative model, the patient's lived experience and the clinician's expertise both shape the treatment pathway. The first step is understanding fit, not imposing a framework.
A plan may include psychotherapy, medication management, integrative wellness support, in-person ketamine evaluation when appropriate, or coordination with existing providers — but the shape of that plan should emerge from a conversation that takes your goals, capacity, and preferences seriously.
At New York Integrative Psychiatry, care is described as collaborative and personalized, aligned with the patient's goals. The practice's role is not to impose a rigid treatment plan but to walk alongside the patient with curiosity, compassion, and clinical expertise. That orientation changes what a first evaluation feels like. It becomes less an examination and more a conversation about fit.
The American Psychiatric Association describes anxiety disorders as highly treatable, with evidence supporting both psychotherapy and, in many cases, medication. But "treatable" is not the same as "one-size-fits-all." Collaborative planning is what makes treatment feel like something that belongs to you — not something being done to you. It is also what helps prevent fragmented care, where anxiety treatment, medication management, and wellness support operate in silos and important information falls through the gaps.
Where Medication, Therapy, Wellness Support, and Ketamine Evaluation May Fit
Not every person who experiences panic escalation needs every option described here. This section clarifies what each dimension of care can involve — not to create a menu, but to reduce the uncertainty that often prevents people from reaching out in the first place.
Psychotherapy
Psychotherapy supports pattern understanding, emotional resilience, and coping — and in anxiety care, that scope matters. It may draw from psychodynamic therapy, cognitive-behavioral approaches, mindfulness-based interventions, or somatic methods, remaining attuned to the broader context of the person's life rather than applying a single protocol uniformly.
For anxiety specifically, psychotherapy can support self-awareness, pattern recognition, and present-day coping. It also creates space to examine the relational, historical, and contextual factors that symptoms alone cannot explain — the kind of work that often matters most in the longer arc of recovery. A relational therapy process can help restore self-trust. Not all anxiety work is about stopping a sensation immediately. Sometimes the work is learning how to stay connected to yourself when sensations appear.
Medication Management
Medication management, in an integrative context, begins with careful evaluation and shared decision-making — not a prescription on the first visit.
A psychiatric medication evaluation may explore current symptoms, medical history, prior medication experiences, side effects, fears, goals, and treatment preferences. The American Psychiatric Association notes that first-line medications for many anxiety disorders can include SSRIs or SNRIs, and that psychotherapy alone may be effective for milder presentations. Any medication decision should be made in consultation with a qualified clinician based on your specific history and circumstances, not on general information in an article.
Medication can feel reassuring to one person and frightening to another. Both reactions deserve room in the conversation. Where medication is no longer needed or no longer serving its purpose, that conversation also belongs in the clinical relationship — a deprescribing orientation that treats medication as a tool rather than a permanent commitment.
Integrative Mental Health and Wellness
Integrative Mental Health & Wellness addresses the dimensions that shape nervous-system regulation: sleep, nutrition, nutraceuticals where clinically relevant, mindfulness practices, stress management, movement, and body-mind integration. These are not complementary add-ons to "real" treatment — they are part of the clinical picture in a whole-person evaluation, because anxiety is lived through the body, not only through thoughts.
This does not mean lifestyle changes replace clinical evaluation. Wellness support is strongest when it is specific, realistic, and connected to the broader care plan. A clinician can help identify which wellness dimensions are most relevant to your particular situation.
Ketamine Evaluation
For some people with treatment-resistant presentations, ketamine evaluation may be a relevant clinical consideration at the appropriate stage, though its use for anxiety and panic disorders is considered off-label. This is not a first-line recommendation for panic or general anxiety, and it does not apply to every person who reaches out.
New York Integrative Psychiatry offers Ketamine Services at its Manhattan office, administered via intramuscular (IM) injection in a supervised clinical setting. Ketamine services are administered strictly in-person and are not available virtually. Ketamine is not automatically relevant to panic escalation or anxiety symptoms, and eligibility is determined through careful clinical evaluation. Where it is relevant, the process involves contraindication screening, preparation, dosing, and integration support. A clinician can assess whether this is a conversation worth having based on your specific history and circumstances.
What This Wider Lens Can Help You Ask Before Reaching Out
Clarity about your own questions is one of the most useful things you can bring into a first clinical conversation. The list below is not a screening tool and it does not produce a diagnosis. It is a set of prompts to help you identify what you are actually trying to understand — so you arrive at that conversation prepared rather than overwhelmed.
- What changed in your functioning after the panic episode — and is that change still happening?
- Are your symptoms repeating, or are you mainly afraid they will repeat?
- Which physical symptoms feel concerning enough to warrant medical evaluation first?
- How have sleep, stress, caffeine, substances, or work pressure shifted in the past several months?
- Have you started avoiding places, plans, commuting situations, or relationships since the escalation?
- What are you most afraid will happen if you reach out for care?
- What do you want treatment to help you understand — not just reduce?
- Do you want to explore therapy, medication evaluation, integrative wellness support, or a coordinated plan?
- What would make a first conversation feel safe enough to have?
There are no right or wrong answers here. The point is not to arrive at a conclusion before speaking with a clinician — it is to arrive at that conversation with a clearer sense of what you are actually asking.
If you reach out to New York Integrative Psychiatry, the intake process allows you to indicate interest in Ketamine Services, Psychiatry/Medication Management, or Therapy. It also includes the option to say "I'm unsure about what I need but would like to find out more." That option exists for a reason. Uncertainty is a valid starting point.
A Gentle Next Step
Panic escalation is disorienting. The aftermath — the questions, the avoidance, the low-grade awareness that something shifted — can be harder to name than the episode itself. That confusion is not a sign of overreacting. It is a reasonable response to a frightening experience, and it is a legitimate reason to seek clarity.
Needing orientation is not the same as being in crisis. It is the beginning of understanding what kind of support might actually fit.
New York Integrative Psychiatry offers a whole-person approach to care through Integrative Psychiatry, psychotherapy, medication management, Integrative Mental Health & Wellness, and other services when clinically appropriate. If you'd like to understand more about how that approach might apply to your situation, Message Us to explore fit.
Text or call 646-859-2339 | 111 W 24th St, Suite 300, New York, NY 10011
Disclaimer: This article is for educational purposes only and is not a diagnosis, treatment plan, emergency guidance, or substitute for care from a licensed medical or mental health professional. If you may be in immediate danger, are experiencing a medical emergency, or are worried you might harm yourself or someone else, call 911 or go to the nearest emergency room. If you are in emotional distress or crisis in the United States, call or text 988 for the Suicide & Crisis Lifeline. In New York City, NYC 988 also offers free, confidential mental health support by phone, text, or chat 24/7/365. New York Integrative Psychiatry is not an emergency resource and does not offer after-hours or emergency assessments. If an emergency arises during or after hours, call 911, go to the nearest emergency room, or use emergency/crisis resources.
About the New York Integrative Psychiatry Insights Team:
The New York Integrative Psychiatry Insights Team is our dedicated engine for synthesizing complex topics into clear, helpful guides. While our content is thoroughly reviewed for clarity and accuracy, it is for informational purposes and should not replace professional advice.